Authors / metadata
Abstract
The prevalence of uterine fibroids of the female genital tract varies from 20–50% in women of the reproductive age group. Surgical management by myomectomy is usually reserved for the nonpregnant uterus. The complication rate in fibroids coexisting with pregnancy may be 10–30%, which are preferably managed conservatively. Red degeneration of fibroids during pregnancy is common, due to the hormonal effect, these in the majority of cases do respond to conservative management. For those not responding to conservative treatment, myomectomy may be an option. Myomectomy in pregnancy remains a controversial issue. Comprehensive peri-operative management is mandatory to minimize complications. A case of a symptomatic uterine fibroids diagnosed during pregnancy was successfully managed by antenatal myomectomy.
Introduction
Uterine fibroids are the commonest benign tumor in women, occurring in approximately 20-30% of women of reproductive age. These are therefore common in pregnancy (1). The prevalence of leiomyomas during pregnancy is reported as approximately 2% (2-4). Although during pregnancy leiomyomas may remain asymptomatic, the surge in placental hormone results in an increase of the fibroid size, this increase may complicate the pregnancy and delivery in several ways; like, increased frequency of spontaneous abortions, fetal growth retardation, preterm labor, premature rupture of membranes, antepartum bleeding, placental abruption, malpresentations, and Cesarean delivery (5,6). Fetal anomalies, namely limb deformities and contractures, may occur as a result of leiomyomas. Myoma usually remain asymptomatic, but the syndrome of “painful myoma”, due to red or carneous degeneration, occurs in approximately 5-8% of myomas in pregnancy (6,7). With adequate analgesia, most pregnancies have a favorable outcome, but in rare circumstances surgical intervention and myomectomy may be required (8).
Justifying myomectomy remains contentious; detailed assessment is important for risk stratification, to identify cases that will be benefitted from surgery and to take preventive steps to minimize complications that can lead to deleterious outcomes.
Case report
A 30-year-old primigravida was referred to the hospital on 12 August 2024 gestational age of 13 weeks 4/7 days with the chief complaint of severe abdominal discomfort for one month. She was diagnosed as a case of uterine fibroid at the eight weeks of gestation when she did complain of severe pain in the abdomen. At that time an ultrasound was done and showed the presence of a myoma of size 7×10.2 cm, with few areas of cystic degeneration. She was being managed conservatively with analgesics and had minimal relief for her symptoms. She was referred to our center for further management. The Patient was admitted to the obstetric ward, on examination her vital parameters were was present, the height of uterus corresponded to 24 weeks of gestation. On vaginal examination the uterus could be felt separately and had a volume of about 12-14 weeks gestational size, beside this, a huge mass of about 15 cm diameter filling the whole abdomen was felt separately. Ultrasonography showed an intrauterine viable fetus of 13 weeks 3/7 days gestation with a large well defined hypoechoic mass arising from the fundus, measuring 7x 14cm cm with a cystic degeneration from right adnexa. As the myoma was fast growing with red degeneration associated with severe pain abdomen, patient was counselled regarding all possible outcomes of pregnancy along with this mass and she agreed to undergo a laparoscopic myomectomy with high-risk consent for spontaneous abortion, blood transfusion and on the rare possibility of hysterectomy.
During laparoscopy, the primary port was placed at the Lee Huang’s point to avoid injury to pregnant uterus and a pneumoperitoneum was created with an intraabdominal pressure of 12 mmHg. On inspection a huge subserosal myoma with a broad base arising from fundus region of the uterus with a size 15x7x7 cm was found along with a 14-week size uterus. Three Secondary ports were placed under direct vision, two on left and one on right. A laparoscopic myomectomy was attempted by coagulation of the base of myoma, but had to be abandoned due to profuse bleeding from the base. The procedure was completed by a laparotomy with a Pfannenstiel incision. Clamps were placed at the base of the myoma and it was removed. Haemostasias was achieved by placing interrupted sutures with Vicryl No 1. Care was taken to avoid taking endometrium in sutures. Fetal monitoring by ultrasonography was carried out immediately after surgery and the fetus was found to be viable. The postoperative period was uneventful and the patient was given tocolysis for 3 days with uterine relaxants and micronized progesterone was continued for four weeks. The patient was discharged on the 7th post operative day, with follow up advice for further antenatal check-ups.
Discussion
Management of uterine myomas in pregnancy, especially those showing degenerative changes, remains controversial as there are concerns of detrimental effects on maternal health and of jeopardizing fetal viability and growth. Generally, conservative management is recommended in uncomplicated cases, however in symptomatic cases showing poor response to medical treatment, an invasive procedure is an option (9-14). The surgical removal of a myoma is generally delayed until after delivery, as mortality and morbidity are slightly higher at myomectomy in the gravid uterus compared to the non- gravid uterus (15). Myomectomy can be considered after comprehensive assessment and counselling to avoid untoward sequelae and the risk of litigation. Myomectomy is justified when there are degenerative changes of the fibroid in pregnancy causing intolerable pain. Heavy bleeding needing transfusion leading to risks of hysterectomy is a major concern in the myomectomy procedure though this was not demonstrated in certain studies (10,11). Additional to the general risks of myomectomy is the risk of abortion which occurs in 18% to 35% of cases¹.
Traditionally, laparoscopic myomectomy in pregnancy is believed to be associated with fetal acidosis, fetal loss and bleeding. This could be due to carbon dioxide retention following pneumoperitoneum at surgery (12). However, laparoscopy has become a trend with successful outcomes (13). A drastic improvement in the learning curve of this technique may have contributed to its popularity. In the present case this treatment method was used initially but was abandoned due to severe bleeding from the base of the fibroid. A meticulous surgery was performed to minimize hemorrhage, with double stitches suturing the peripheral feeding vessels. Haemostasias was secured before closure. As progesterone calms the myometrial activity and prevents premature labor, its use is strongly recommended. Large meta-analyses significantly revealed a reduction of premature birth before 34 weeks in high-risk cases (14-16). Mollica et al. (17) conducted a prospective study of 106 pregnant women with uterine myomas who were admitted with recurrent abdominal pain. This study shows that regardless of gestational age, the outcomes for all women who underwent myomectomy (n=18) was superior to those managed conservatively in terms of pregnancy loss (0% versus 13.6%), premature rupture of membranes (5.6% versus 22.7%), preterm labour (5.6% versus 21.6%) and post-Cesarean hysterectomy (0% versus 4.5%). However, in patients like our own a timely and well-planned myomectomy can be an option offered to the patient, avoiding morbidity and mortality associated with the myoma.
Conclusion
The decision to perform a myomectomy during pregnancy should be based upon the symptoms, failed medical management, fibroid size, its location and its rapid growth to prevent various possible forthcoming adverse events. Therefore, a carefully planned myomectomy in huge myomas in selected cases is an appropriate low morbidity option which can be offered to the patient.
References
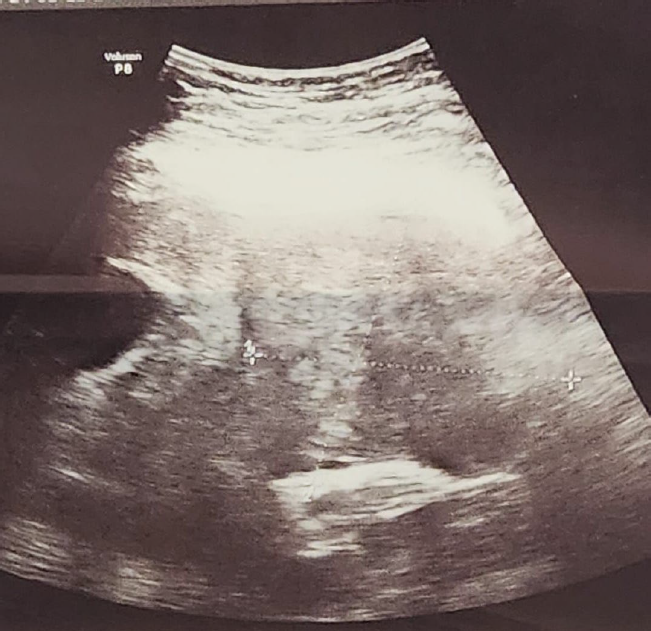
Figure 1: Ultrasound of the myoma with necrotic zones.

Figure 2: Ultrasound of the mass filling the abdomen.

Figure 3: Dimensions of the myoma.



