Affiliation: 1: Department of gynecology and Minimally Invasive Unit, Vita Batel Hospital, Curitiba, Paraná, Brazil
2: Division of Minimally Invasive Gynecologic Surgery, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville, Florida, United States
The surgical technique is essential to adequately manage the disease. The objective of this video is to show a meticulous technique to be necessary to adequately manage of Laparoscopic cystectomy for the treatment of ovarian endometrioma. This video reports in detail our current technique for laparoscopic cystectomy for ovarian endometrioma and all the tricks to permit a good answer to reproduction, and even improvement of the technique by other surgeons.
Objective
To describe a reproducible safe laparoscopic technique for the excision of ovarian endometriomas.
Design
Video presentation.
Case report
Perfect surgical technique and knowledge of the anatomy is essential to adequately excise endometriosis. The ovarian endometrioma may be found in up to 44% of women with endometriosis. The steps of a laparoscopic ovarian cystectomy for ovarian endometriomas are described in this video utilizing a reproducible technique with the aim of reducing trauma to ovarian injury. 10 key steps are highlighted.
Step 1: Patient preparation and establishment of peritoneum.
Step 2: Use of uterine manipulator
Step 3: Systematic diagnostic laparoscopy, endometriotic lesions mapping, and ovariolysis
Step 4: Aspiration and irrigation of endometriotic cyst contents.
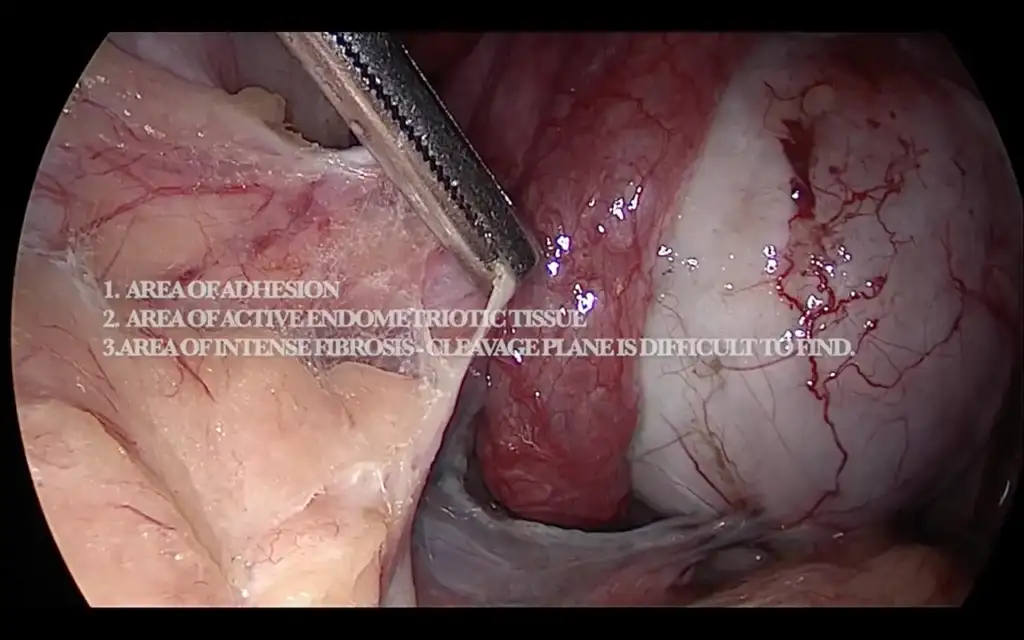
Step 5: Identification of the endometrioma cleavage plane.
Step 6: Dissection of the ovarian endometrioma utilizing divergent forces
Step 7: Dissection of the deep aspect of the endometrioma near the ovarian hilum.
Step 8: Hemostasis.
Step 9: Excision of broad ligament and pelvic sidewall peritoneum.
Step 10: Extraction
Video
Conclusion
The ovarian endometrioma is seen in up to 44% of women with endometriosis. Premature surgical menopause and decreased anti-Mullerian hormone (AMH) after ovarian cystectomy is a concern that must be discussed with patients.
References
1. Cranney R, Condous G, Reid S. An update on the diagnosis, surgical management, and fertility outcomes for women with endometrioma. Acta Obstet Gynecol Scand. 2017Jun;96(6):633-643. doi: 10.1111/aogs.13114. Epub 2017 Mar 11. PMID: 28186620.
2. J Turk Ger Gynecol Assoc. Ovarian cystectomy in endometriomas: Combined approach2014; 15(3): 177–189.Published online 2014 Sep 1. doi: 10.5152/jtgga.2014.1111.
3. Kondo W, Ribeiro R, Tripia C, Zomer MT. Deep infiltrating endometriosis: anatomical distribution and surgical treatment. Rev Bras Ginecol Obstet. 2012;34(6):278-84.
4. Busacca M, Riparini J, failure Somigliana E, Oggioni G, Izzo S, Vignali M, Candiani M. Postsurgical ovarian after laparoscopic excision of bilateral endometriomas. Am J Obstet Gynecol. 2006 Aug;195(2):421-5. doi: 10.1016/j.ajog.2006.03.064. Epub 2006 May 8. PMID: 16681984.
5. Redwine DB. Ovarian endometriosis: a marker for more extensive pelvic and intestinal disease. Fertil Steril. 1999 Aug;72(2):310-5. doi: 10.1016/s0015- 0282(99)00211-3. PMID: 10439002
6. Chapron, C. et al. Associated ovarian endometrioma is a marker for greater severity of deeply infiltrating endometriosis. Fertil. Steril. 92, 453–457 (2009) endometriomas. Fertil Steril 82: 1633-7 (2004)
Open access: These articles are distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.