Authors / metadata
DOI: 10.36205/trocar5. vid24007
Abstract
Deep endometriosis is characterized by the infiltration of endometriotic tissue beyond the peritoneum, affecting not only reproductive organs but also nearby structures, including the intestinal tract. Surgical management becomes particularly challenging when the disease infiltrates the rectosigmoid colon, often requiring advanced surgical interventions. Intestinal surgical approaches, including segmental and discoid resections, are associated with significant risks and complications. The well-known and previously published “En Bloc Hysterectomy Technique” describes the simultaneous hysterectomy and the affected portion of the rectosigmoid through a segmental resection. This video article introduces a novel surgical approach, the ‘Modified En Bloc Hysterectomy’, designed for cases requiring hysterectomy with concurrent intestinal involvement classified as #Enzian C2. The ´Modified En Bloc Hysterectomy´ technique allows for simultaneous hysterectomy and intestinal discoid resections, enhancing intestinal-sparing surgery in patients where radical intestinal resection is not required. This surgical approach reduces the risk of complications by allowing dissection and visualization of healthy structures before reaching compromised areas. This reduces the risk of fistula formation and intestinal injury during surgery, as well as reducing overall intraoperative time.
Learning Objective: The present video aims to demonstrate the advantages of the ´Modified En Bloc Hysterectomy´ for deep endometriosis with intestinal involvement.
Introduction
Deep endometriosis is characterized by the presence of endometrial-like tissue infiltrating beyond the superficial peritoneum. It is a complex disease that affects not only the reproductive organs but also adjacent structures such as the intestinal tract. It is estimated that between 5% to 37% of patients with deep endometriosis present involvement of the rectosigmoid, being one of the most common extragenital locations. This condition not only causes severe pelvic pain but can also trigger severe digestive symptoms such as constipation, pain during bowel movements, and, in some cases, partial bowel obstruction. These surgeries present high complication risks, reaching 10–22% when colorectal resection is required. This is why these procedures should be carried out by highly trained surgeons with extensive knowledge of pelvic anatomy. The surgical approach when the intestine is compromised by endometriosis will depend on different factors such as the size of the lesion and the extent and depth of the wall involvement. Different strategies may be considered, ranging from conservative techniques such as rectal shaving, discoid resections, or a radical approach such as segmental resection.
Patient and Methods
We present a case of a 40-year-old patient with symptoms of dysmenorrhea, chronic pelvic pain, dyschezia, and severe dyspareunia. Mandatory pre-surgical endometriosis mapping was realized, and the pelvic MRI findings revealed a 25mm nodular plate involving the uterine isthmus, retraction of the posterior vaginal fornix, and ovaries pulled toward the midline; bilateral endometriomas, three cm on the right side and five cm on the left side. An intramural endometriotic nodule of the rectum measuring 26 mm and located ten cm from the recto-anal junction. Diffuse posterior adenomyosis. #Enzian Classification: P0, O2/2, T3/3, A2, B2/2, C2, FA.
Main Outcomes
Surgery lasted 158 minutes. The patient was monitored during hospitalization with vital signs, procalcitonin and C-reactive protein levels, as a parameter of colorectal anastomosis dehiscence, which remained within normal values. The patient was discharged from the hospital with adequate tolerance to a general anti-inflammatory diet after the second day of hospitalization, with no further complications.
Results
The patient showed significant improvement of symptoms one month after surgery, along with an anti-inflammatory nutritional plan. Pathological anatomy revealed: Uterus with extensive diffuse adenomyosis; colonic muscular layer with chronic inflammation and edema, associated with a fibromuscular tissue nodule with endometriosis.
Thematic considerations
As mentioned earlier, in our strategy the intestinal approach will depend on the size of the lesion and the extent of the intestinal wall involvement. The discoid resection involves the excision of a disc-shaped portion of the anterior wall of the bowel. This procedure is mainly used for deep but localized lesions, #Enzian C1-C2, meaning less than three centimeters in size. This technique is associated with less morbidity compared to segmental resections. Instead of removing a full intestinal segment, a disc of affected tissue is excised, minimizing damage to the intestinal structures, and preserving function. It allows for a quicker recovery with a lower risk of complications such as infections and postoperative obstructions. The segmental resection technique is used when the disease significantly affects a large portion of the bowel circumference, #Enzian C3, or when there are multiple deep lesions, meaning a multifocal disease. In this case, a complete intestinal segment is removed, and a primary anastomosis is performed to reconnect the healthy ends. Segmental resection carries a higher risk of complications, such as fistulas or dehiscence.
According to the strategy of our center, intestinal endometriosis surgery, the priority is to adopt a conservative approach, aiming to preserve intestinal function. However, this approach is valid only if the complete removal of the disease can be ensured. Residual endometriotic tissue leads to persistence of the pathologic tissue, rising the risk of recurrence of symptoms and therefore, worsening the patient’s quality of life. Thus, the surgical intervention applied to each patient is carefully evaluated based on the severity of the intestinal involvement, being therefore, an individualized decision. The Video Article “A novel Technique for En Bloc Hysterectomy in the Treatment of Deep Endometriosis #Enzian C3 Bowel Nodules” published in 2023 by Cabrera R and Kondo W describes the “EBH” technique for the treatment of deep endometriosis with rectosigmoid involvement, specifically #Enzian C3 nodules.
This technique involves the simultaneous resection of the uterus and the affected portion of the rectosigmoid through a segmental resection, reducing surgical time and providing a more efficient approach. The benefit of “EBH” technique is that it reduces the risk of complications by first accessing healthy planes of the recto vaginal space, until the clear visualization of the Denonvillier’s fascia, before heading to the compromised areas, as it is clearly exposed in the Video. This ensures better visualization and careful separation of the structures, minimizing the risk of intestinal injury during the dissection. To perform “EBH” technique certain criteria must be met such as ensuring that the intestinal nodule is at least seven centimeters from the anal margin. This is because a sufficient healthy distal margin is needed to create the stapler line below the nodule. In this article, we developed a `Modified En Bloc Hysterectomy´ technique, as we are performing a hysterectomy combined with a conservative procedure, such as discoid resection instead of a segmental resection. Although the surgery applies an En Bloc approach until the step of the anterior colpotomy with the intestinal nodule adhered to the retro-uterine surface; once the healthy space of the rectovaginal septum is dissected and identified between the retro-uterine surface and the bowel, the uterus is carefully separated from the intestine, allowing to perform a discoid resection of the affected bowel. This modified technique allows for intestinal-sparing surgery in patients where radical intestinal resection is not required, while still maintaining the previously and already published benefits of En Bloc Hysterectomy for deep endometriosis surgery.
Conclusion
The ´Modified En Bloc Hysterectomy´ technique seems to offer an effective, low-risk surgical approach for patients with deep endometriosis and intestinal involvement classified as #Enzian C1-C2. This technique emphasizes the preservation of function and minimizes complications, ensuring better visualization of vital structures, and significantly reducing intraoperative time. It is a promising option for cases of deep endometriosis that require intestinal resection.
Comment by Editor: We are publishing the surgical strategy shown by the authors because it appears to be a new and practical approach. However, we would like to point out that there is no study data on this and that this is a case report. We look forward to see further research on the publish strategy.
Video
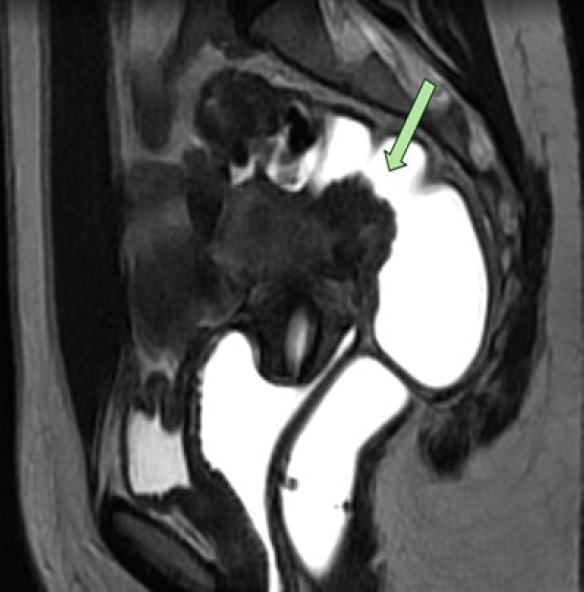
Figure 1: The intestinal nodule can be visualized located ten cm from the anal margin, measuring approximately 26 mm in diameter, with involvement of the rectal wall’s muscular layer.
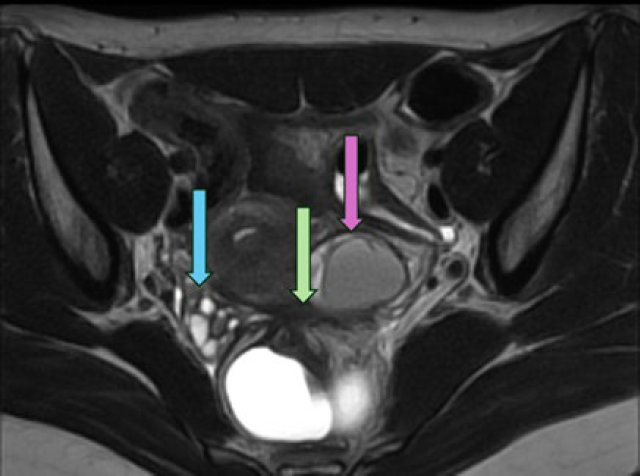
Figure 2: The pink arrow indicates a five cm endometrioma on the left ovary, with minimal healthy parenchyma remaining. The blue arrow points to multiple endometriomas in the right ovary. Both ovaries are retracted towards the midline. The green arrow indicates the retro cervical nodule that pulls the aforementioned structures and the rectosigmoid at that level.