Authors / metadata
DOI: 10.36205/trocar5.2024016
Abstract
Leiomyomas are benign mesenchymal tumours which originate usually from smooth muscle cells, hence can arise at any site where smooth muscle cells exist. In females, most commonly seen in uterus, extra uterine leiomyomas are rare and seldom found in the space of Retzius. The authors report a rare case of a large retropubic leiomyoma in a 45-year-old lady who presented with urinary symptoms and abnormal uterine bleeding. Clinical examination and imaging showed a uterine leiomyoma with a doubtful urethral leiomyoma. It was approached laparoscopically and excision of the mass was performed in toto along with a total laparoscopic hysterectomy. Very few cases have been reported in the literature so far. Histopathology showed a benign leiomyoma similar to the uterine counterpart.
Introduction
Uterine leiomyomas are the most common benign neoplasm of the female genital tract. It affects 25% to 30% of women in reproductive age group. However, extra uterine leiomyomas are a rare entity and can arise at nearly any anatomical site and hence these become a diagnostic challenge. Histologically those are benign smooth muscle tumours similar to the uterine counterparts and usually arise at the genitourinary tract like vulva, vagina, urethra, bladder and rarely in the retroperitoneum. The incidence of leiomyoma among all retro peritoneal tumours is only 1.2% (1) Retroperitoneal leiomyomas are commonly found in the posterior retroperitoneum rather than in the anterior retroperitoneum including the Retzius space (2). The space of Retzius is an anatomical virtual space bounded anteriorly by the pubic bone and posteriorly by the bladder. In the literature only few leiomyomas have been reported at the space of Retzius. A leiomyoma in this location remains asymptomatic until it becomes large enough to cause urinary symptoms and pelvic pain.
Case Report
A 45-year-old female presented to the center with complaints of heavy menstrual bleeding and urinary symptoms including increased frequency and incomplete evacuation of the bladder over the last four months. She was a known case of histopathological proven fibroadenoma of the right breast and a fibroid uterus but lost to follow up. General and systemic examination were within normal limits. On bimanual pelvic examination the uterus was irregularly enlarged and corresponded to a 16 weeks gravid uterus, mobile with free fornices. A mobile mass of size eight by eight (8x 8) cm was felt through the anterior vaginal wall in the retropubic region, and the vaginal mucosa was felt free moving over the mass. MRI pelvis revealed a T2 hypointense lesion measuring 7.5×5.8×6.8cm seen anterior to the vagina beneath the bladder base compressing the vagina. The lesion was seen separate from the anterior wall of cervix, but the anterior wall of the urethra could not be identified separately (Fig 1).
Minimal internal cystic degeneration was seen and the uterus was enlarged with multiple myomas the largest being 3.3cmx2.8cmx2.3cm. Total laparoscopic hysterectomy with excision of the mass and bilateral ureteric stenting was planned. Intraoperatively the above-described mass could not be approached after reflecting the bladder off the uterus and was found to be anterior to the bladder in the retropubic region. Hence it was approached through the space of Retzius and was found to be an encapsulated tumor arising in this area with no connection to the adjacent organs, no feeding vessel was found and the mass was removed in its entirety (Fig 2).
The removal of the mass was followed by a total laparoscopic hysterectomy with bilateral salpingectomy. The specimen was retrieved in a later phase by en-bag morcellation. Post operatively the patient recovered well. Histopathology revealed typical features of benign leiomyoma (Fig 3).
Discussion
Extra uterine leiomyomas are a rare entity with complex pathogenesis and the diagnosis and management of which can be challenging. Even though leiomyomas are classically described to be arising from uterine smooth muscle, they can arise as a result of clonal proliferation of such cells at any anatomical sites. In addition, unusual growth patterns are seen, benign metastasizing leiomyoma, intravenous leiomyomatosis, disseminated peritoneal leiomyomatosis, parasitic leiomyoma and retro peritoneal growth. Only 15 % to 20% of all retroperitoneal tumours are benign, fewer than half are sarcomas and the remaining are primary lymphomas or other malignancies. Leiomyomas of retroperitoneum accounts to only for 1.2% of detected leiomyomas 73% occur in the pelvis minor and less than 1% in the broad ligament (1). The space of Retzius is a part of the extra peritoneal space located between the transversalis facia of the abdominal wall and the parietal peritoneum, bounded by the pubic bone anteriorly and the urinary bladder posteriorly. The floor of this space is delineated by the pubo vesical ligament and Santorini’s retropubic venous plexus. It is also referred to as retropubic, antero vesical space, cave of Retzius: the Retzius space. It is also a surgical landmark for gynaecological surgeries like sling operations for urinary incontinence, Burch colposuspension and non gynaecological surgeries like hernia repair. True tumours in the Retzius space are seldom found. Only 10 cases of leiomyoma have been reported in females in the literature (3-6). Of which one was tackled laparoscopically (7) and one was a robotic assisted laparoscopic excision (8). Other rare tumours which arise in space of Retzius are cellular angiofibroma, cystic lymphangioma, spindle cell tumor and non-neoplastic conditions like abscess and hematomas.
Although the most important differential diagnosis of leiomyoma in retroperitoneal space is leiomyosarcoma, no case has been reported yet in the space of Retzius. Table 1 lists the reported leiomyoma in literature.
Various theories have been postulated by different researchers on the etiology of leiomyomas arising in retroperitoneal space. Kho et al. suggested a iatrogenic etiology as they observed 83% of them with leiomyomas both extra peritoneally and intra peritoneally had a history of abdominal surgeries and 67% of them had undergone laparoscopic myomectomies with morcellation (9). Other authors stated that extraperitoneal leiomyomas arise from the remnants of Mullerian or Wolffian ducts or from the smooth muscles of vascular walls (10). In 40% of cases, leiomyomas co-exist with uterine myomas or can be related to past hysterectomies (2).
A clinical challenge will be to precisely locate the tumor in the retroperitoneal space and to differentiate it from malignant neoplasms. Even though 100% accuracy is deniable, MRI / CT Pelvis can locate and rule out malignancy to a great extent. Preoperative transdermal biopsy and histopathology can help in obtaining accurate diagnosis;
however, it could expose the patients to malignant cells if not benign. In the presented case, the pre operative diagnosis was doubtful of vaginal leiomyoma or urethral leiomyoma as the location was thought to be between the vagina and the urethra, and it was coexistent with uterine leiomyomas. Even though an MRI was taken pre operatively, the origin could not be precisely made out. Since it was co existent with uterine myomas and imaging showed no suspicion of malignancy, a laparoscopy was decided on. A leiomyoma from the retropubic space was removed in toto as it had no attachment eighter to the uterus nor to the bladder followed by a hysterectomy with bilateral salpingectomy. Histopathological examination revealed a benign leiomyoma from the space of Retzius and enlarged uterus with leiomyomas.
Conclusion
In case of patients presenting with urinary symptoms, differential diagnosis including tumours in the extraperitoneal space should also be considered including in the space of Retzius. Especially when the patient is presenting with uterine leiomyomas. Imagining diagnostics including MRI helps in locating and ruling out features of malignancy and to have a structured surgical plan. A leiomyoma in the space of Retzius has to be surgically removed completely and with good knowledge of the anatomy, this can be safely done laparoscopically.
References
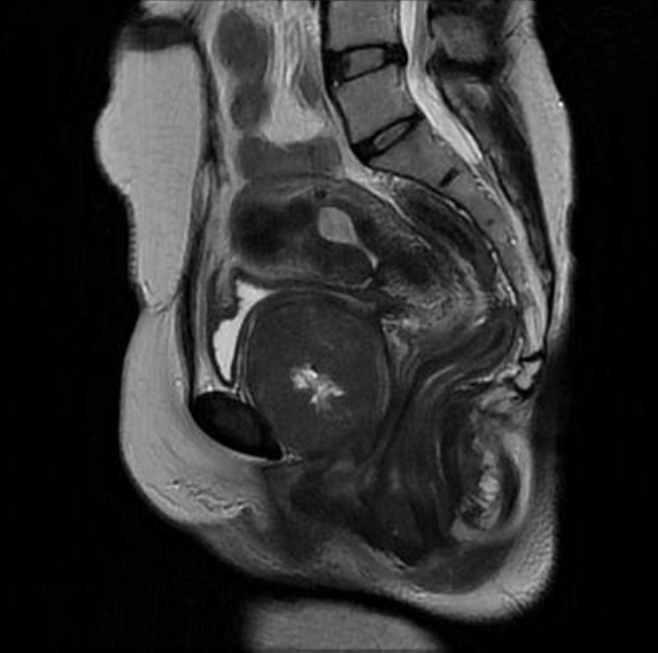
Fig.1: MRI imaging showing leiomyoma anterior to the cervix and anterior vaginal wall

Fig. 2: Intraoperative picture showing large leiomyoma in retro-public space (Space of Retzius)
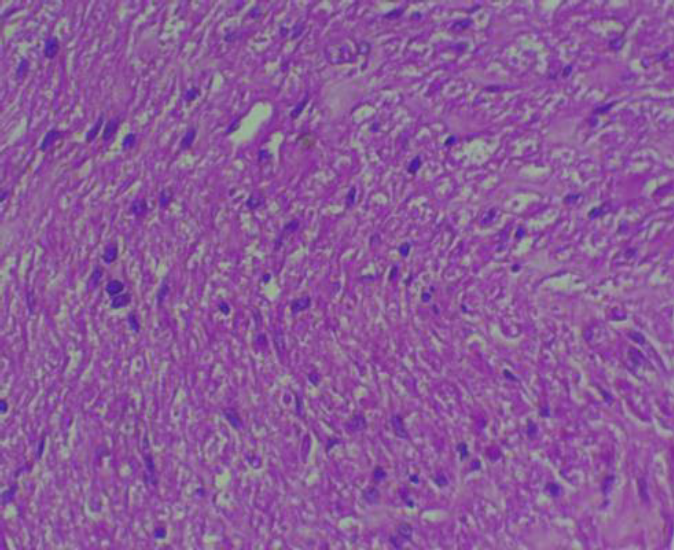
Fig. 3: Histopathology showing leiomyoma cellular pattern similar to uterine leiomyoma
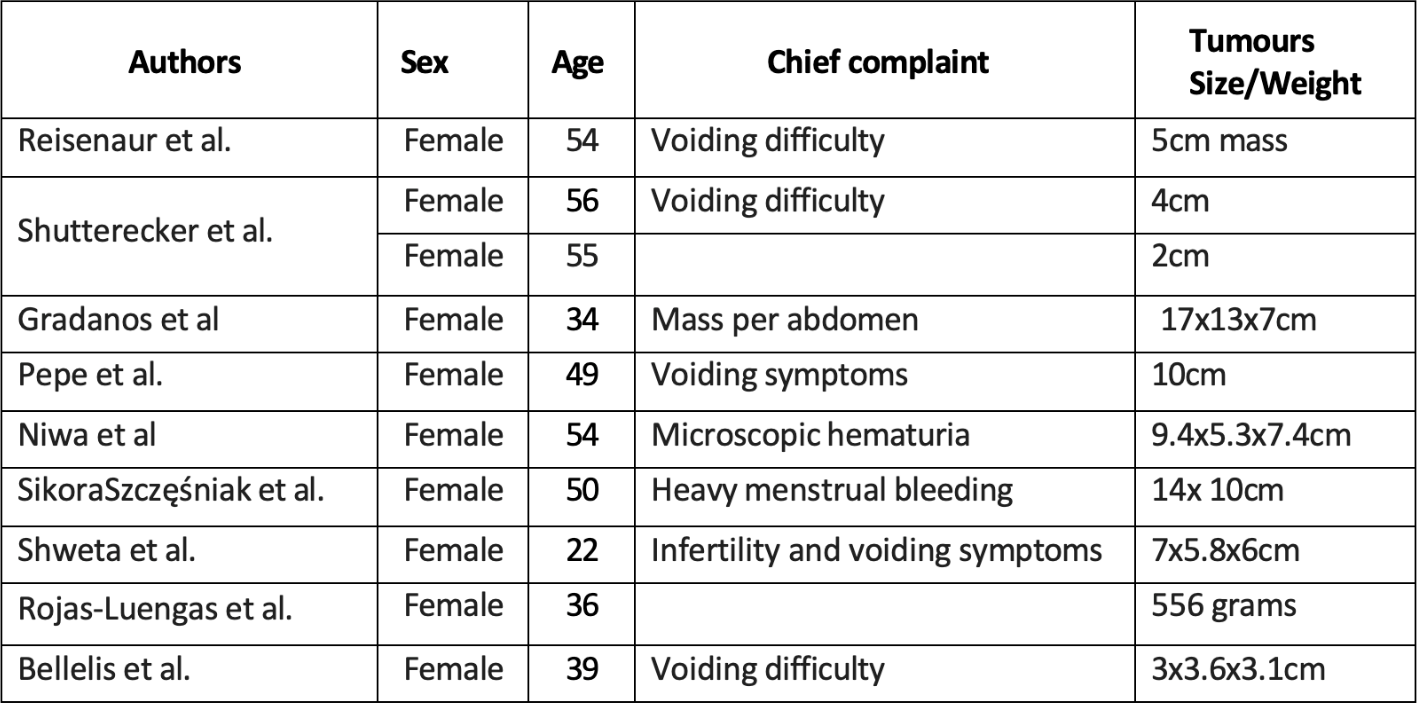
Tab 1. Listing the complaints and tumor size/weight in literature.



