Authors / metadata
DOI: 10.36205/trocarvid5.24003
Abstract
Objective: A rare case scenario of Transperitoneal migration of Spermatozoa with Ruptured Ectopic gestation in a Unicornuate uterus (U4b)– A Case report.
Design: Retrospective study – review of surgical procedure.
Setting: Patient consent was taken. She was operated at a hospital in Mumbai. Procedure was done under general anaesthesia. Port configuration used was 1 supra umbilical 10 mm port for optics and 2 left sided ipsilateral 5 mm accessory ports for the surgery.
Intervention: Laparoscopic right salpingectomy with drainage of the hemoperitoneum.
Conclusion: Demonstrating the laparoscopic findings in this rare case of ruptured tubal ectopic gestation and establishing evidence-based findings of transperitoneal migration of spermatozoa leading to ectopic gestation in the contralateral tube.
Introduction
This case report describes a case of Transperitoneal migration of spermatozoa leading to an ectopic gestation. The patient is a 29-year-old, Gravida 1 Para 0, Married for 2 years, no previous abortions or living issues. She has not had any prior scans so is unaware of the congenital mullerian anomaly which had not been diagnosed prior to this episode of ruptured tubal ectopic pregnancy.
The patient had a congenital uterine anomaly of class U4b with Left sided Unicornuate uterus and the ectopic gestation was noted in the Right tube (on the side of the undeveloped uterine horn) which subsequently ruptured causing hemoperitoneum (as is seen in figure 1 and 2). The patient underwent an emergency laparoscopic salpingectomy. (as is seen in Figure 3). The patient was a 32-year-old with complaints of severe abdominal pain for 1 day and bleeding vaginally.
She had history of 6 weeks amenorrhea and a positive Urine pregnancy test. A 3D ultrasound confirmed the findings of a ruptured right tubal ectopic gestation with hemoperitoneum and a Mullerian anomaly of class U4b (Unicornuate uterus on the left side).
She was taken up for emergency Laparoscopic salpingectomy under general anesthesia and the Intra operative findings confirmed the diagnosis (Operative pictures attached)- as is seen in figure 4. This suggests a pathogenesis of transperitoneal migration of sperm as has been recorded previously in literature as cited below. The right sided salpingectomy was performed and final histopathology of the specimen confirmed the diagnosis of an ectopic pregnancy.
The pathophysiology as suggested by the authors is that the sperms transmigrated through the uterus into the left patent fallopian tube and through the peritoneum to fertilize the ovum in the right sided fallopian tube to then lead to an ectopic pregnancy in the right tube as there is no direct pathway to the uterus from the right fallopian tube. The ovulation however could have occurred from either side as the ovum could be released into the pouch of Douglas in the peritoneal free fluid and then picked up by the sweeping motion of the fimbria of the right fallopian tube to then implant in the tubal epithelium. This appears to be the only logical explanation for occurrence of this rare phenomena as seen in this case report.
Review of literature
This case represents the phenomenon of contralateral sperm transperitoneal migration: sperm gaining access to the left oviduct after entering the peritoneal cavity via the right oviduct. The ovum from the left ovary after being successfully fertilized could not be transported into the uterine cavity due to the previous segmental resection, ultimately resulting in an ectopic pregnancy. [1]
Intraperitoneal sperm transmigration occurs approximately half the time in effecting spontaneous human pregnancies. To minimize the risk of ectopic tubal pregnancy in woman with unilaterally damaged fallopian tubes, salpingectomy should be the preferred surgical treatment, rather than attempting tubal salvage and repair.[2]
This is the first report of an intrauterine pregnancy following timed coitus, resulting from transperitoneal sperm and/or oocyte migration as the oocyte originated from an ectopic (undescended) ovary. [3]
The occurrence of ectopic pregnancy distal to complete tubal occlusion or separation (in a tubal segment without luminal continuity to the uterus) was explored among reported tubal pregnancies, particularly those following sterilization. Presumably such pregnancies result from transperitoneal migration of sperm.
Pregnancy occurring in a tubal segment without luminal continuity to the uterus without prior sterilization was only rarely reported.[4]
Congenital mullerian anomalies and their classification.
Video
References
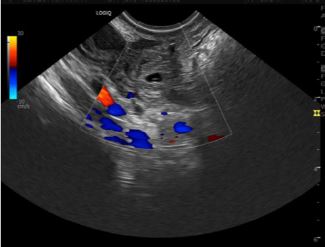
Figure 1: Ultrasound image of the tubal ectopic gestation in the right tube
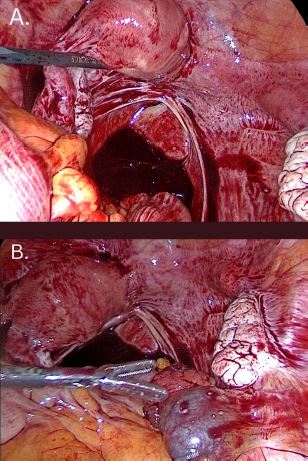
Figure 2
A)Shows the initial operative pictureclearly demonstrating the Rupturedtubal ectopic gestation withHemoperitoneum in the Pouch ofDouglas. The Mullerian anomaly canbe clearly identified and is seen as anormal well developed uterine horn onthe left side with a normal left adnexalcomplex. The Right side howeverdemonstrates absent uterus withrudimentary undeveloped horn and nocavity.
B)The right ovary is normal and the rightsided tube shows the ectopic gestationof size about 3×4 cm with activehaemorrhage through the fimbrial end.The Cornual side of the tube does notshow any communication with theuterus suggesting an Etiopathogenesisof transperitoneal migration of theSperm to then undergo implantation ofthe embryo in the right tube
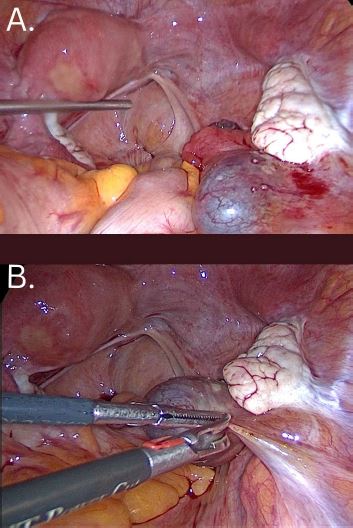
Figure 3
A Shows the laparoscopic view after giving a saline wash. B Findings were confirmed and Right salpingectomy was done using standard
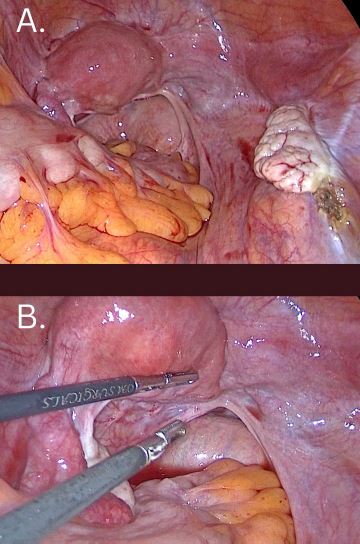
Figure 4
A-Shows the final operative picture aftersalpingectomy and thorough saline lavage.
B-The Unicornuate uterus is clearly visiblewith the rudimentary undeveloped horn onthe right side. The specimen of the righttube was sent for histopathology andconfirmed the diagnosis of ectopicpregnancy in the right tube.



