Authors / metadata
DOI: 10.36205/trocar5.2024004
Abstract
As a gynecologist many diagnoses come to mind when being presented with a 36-year-old patient with a large unilocular anechoic cyst in the pelvis. One diagnosis which should be added to that list, though being rare and not anatomically linked to the genital organs, is a chylous mesenteric cyst. This case report reflects upon available published data and presents a case of this rather seldom and unexpected condition.
Introduction
Chylous cysts are a rare occurrence and even more so in the field of gynecology. Predominantly it emerges from the mesentery of the small intestines, but can result from any part between the duodenum and rectum. Incidence settles at 1 in 100,000 patients. The pathogenesis has not yet been determined and the condition can present with a number of unspecific symptoms of the lower abdomen. (1) Preoperative diagnostics frequently reveal a unilocular anechoic cyst of unknown origin which can change position in imaging techniques such as ultrasound and CT-scan. (2)
Case description
36-year-old female patient, no pre-existing illnesses, no previous operations on the abdomen, two previous pregnancies and following vaginal deliveries, regular check-ups with gynecologist without previously noted abnormalities.
According to the patient first symptoms such as cramps and feeling of pressure in the lower and middle abdomen and the inability to stand for extended periods of time, due to severe back pain in thoracic and lumbar region, presented approximately two months before the diagnostic laparoscopy.
One month before the procedure, the patient was admitted to the orthopaedic department of a different hospital with severe back pain, during which a CT-scan was administered which revealed a large cyst in the abdomen of unclear origin.
A follow-up appointment was made with her gynecologist who suggested a diagnostic laparoscopy assuming the anechoic round structure, in close proximity to the inconspicuous ovaries, could be a paraovarian cyst (see ultrasound pictures 1,2 and 3 below).
When entering the abdomen at laparoscopy the pelvis was predominated by an approximately 10 cm in diameter round structure. When initiating
Trendelenburg position the previously mentioned structure relocated to the middle to upper abdomen.
The described structure was vulnerable to touch by surgical instruments. A milky low-viscous fluid was released (see picture 7 below) and upon close inspection it became clear the cyst was connected to the mesentery of the small bowel. The small connection (see picture 6) was ligated and cut via endoscopic stapler. The cyst was removed via endoscopic plastic bag. The pathological exam confirmed clinical diagnosis.
The postoperative period concluded without any complications and the abdominal surgical drain which had been inserted into the abdomen as precautionary measure was removed on day two after surgery and the patient was discharged.
Discussion
Despite literature indicating that chylous cysts are a condition more frequently associated with male patients and also more commonly diagnosed in the fifth decade of life, there are many similarities when comparing the presented patient who is a female in her thirties with other case reports. (3), (4), (5) Therefore chylous cysts should be added to the list of differential diagnoses that need to be considered in the gynecological field when treating patients with abdominal cysts of unknown origin.
References
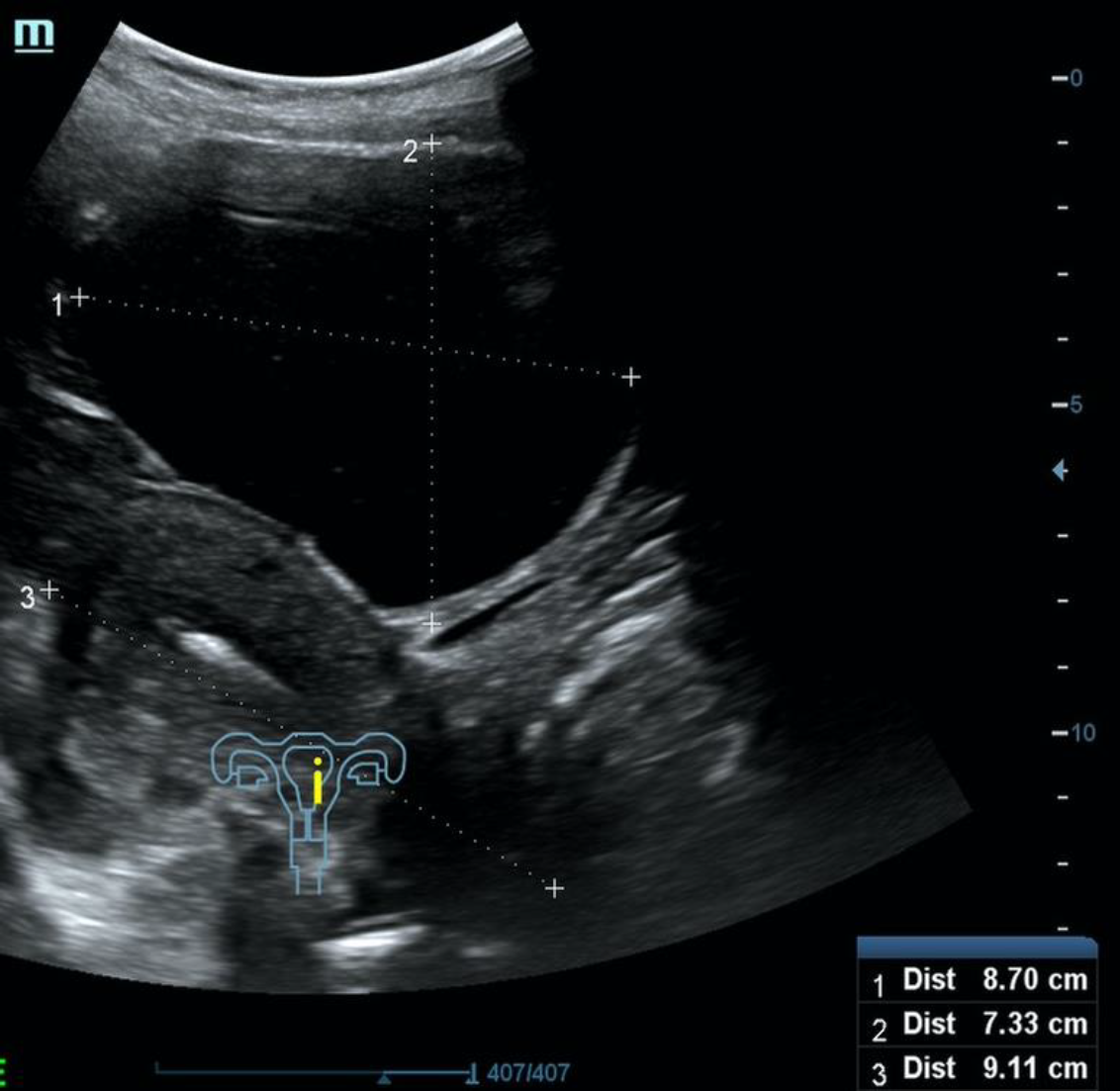
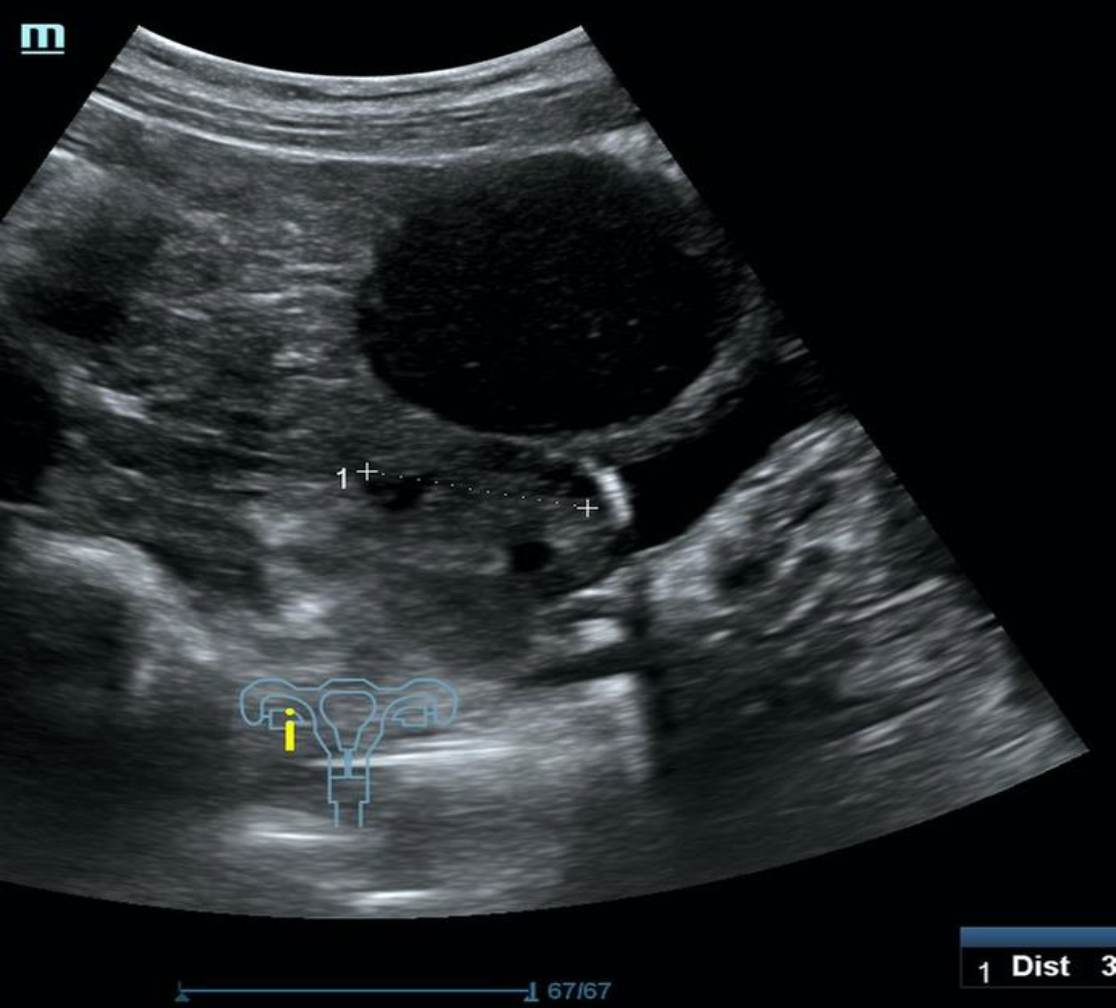
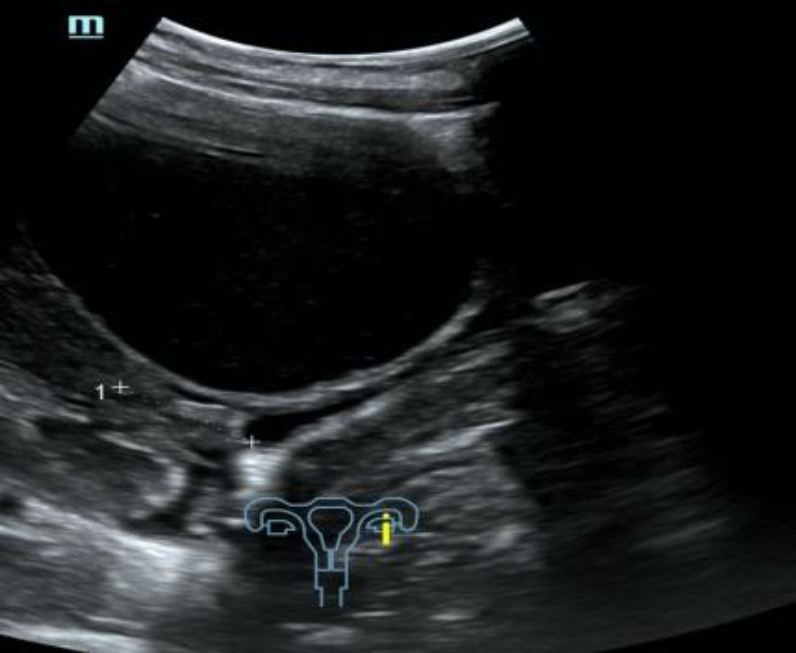
Ultrasound view Picture 1-3

Picture 4: First sighting when entering the abdomen laparoscopically
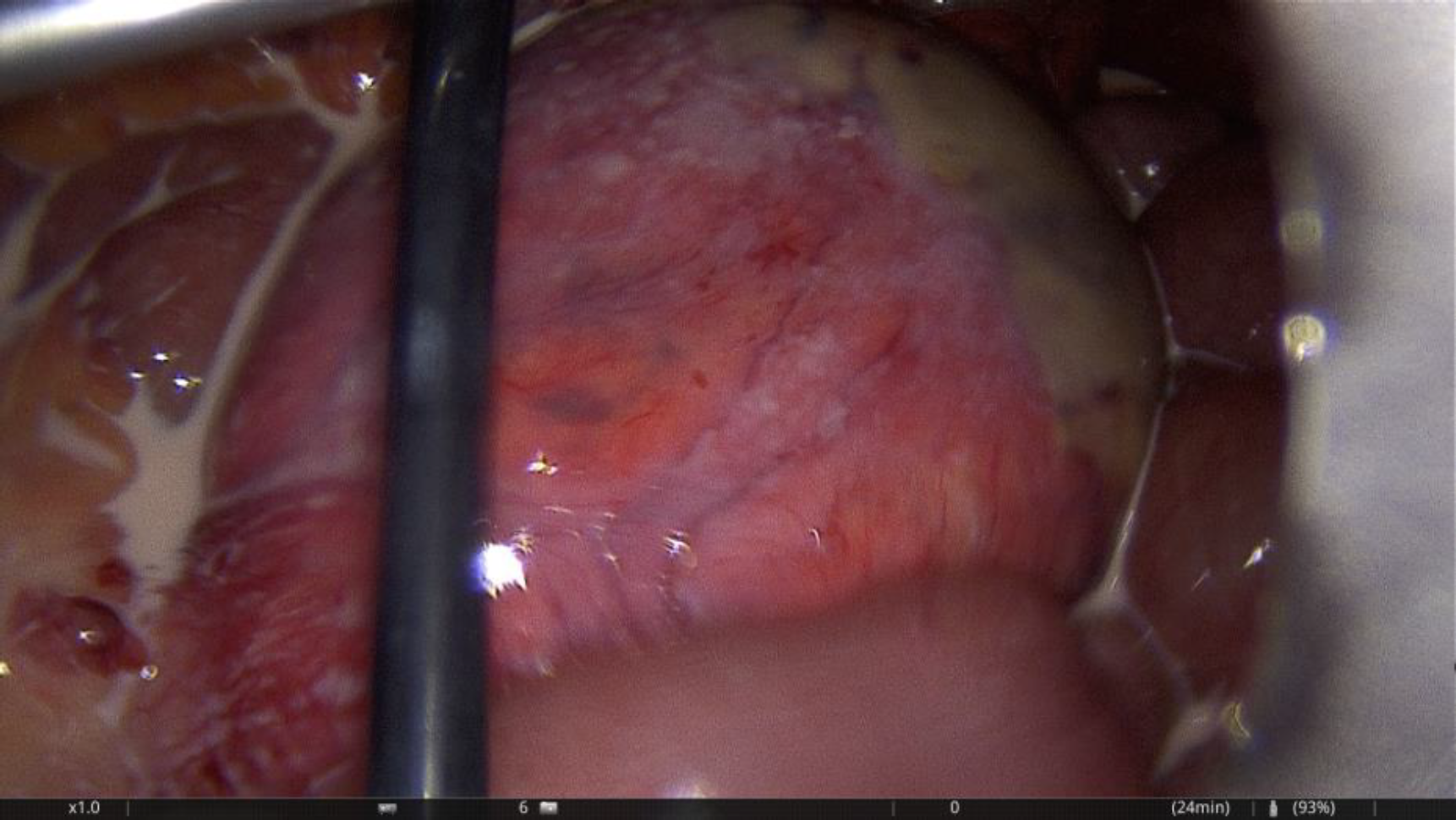

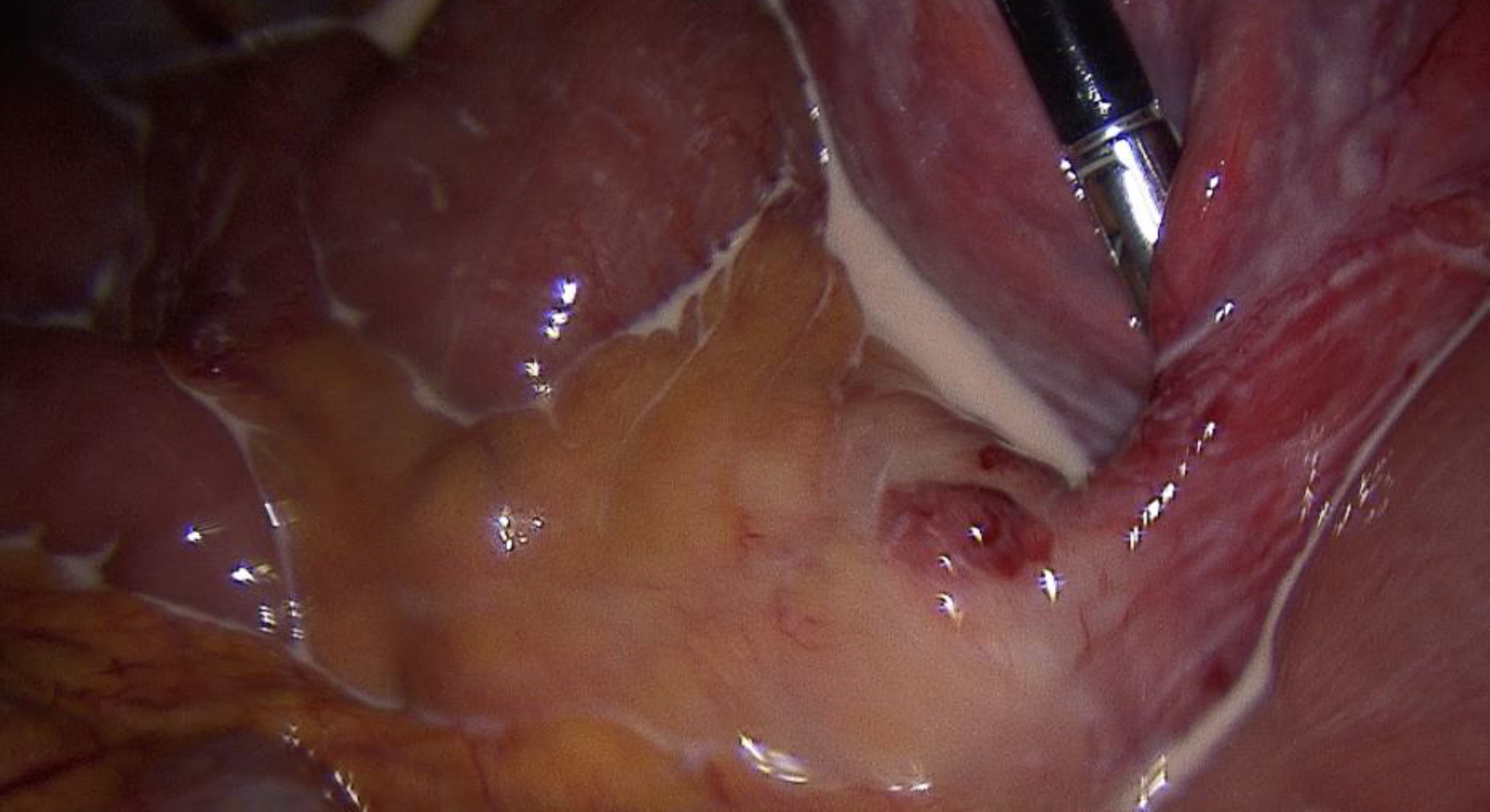
Pictures 5,6 & 7: First one showing the whole extend of the cyst, middle one showing the connection between the chylous cyst and the mesentery go the smaller intestine and the lower one showing the milky-fatty fluid which erupted from the cyst



