Authors / metadata
DOI: 10.36205/trocar1.2021003
Abstract
Intrauterine retention of fetal bones is a rare complication of unsafe abortion that can cause secondary infertility. We are presenting the case of a young woman who underwent an illegal abortion 4 years ago. Transvaginal ultrasonography suggested the presence of bone-like structures in the uterine cavity. Retained bony structure from a previous abortion should be considered as a cause of secondary infertility. Removal of the bony products and polypectomy was done by hysteroscopy.
Corresponding author: Ameneh Haghgoo, email: mnhaghgoo@yahoo.com
Introduction
Bone within the uterine cavity is an unusual finding in women with secondary infertility, which is usually associated with a past history of termination of pregnancy. The etiology of bone like calcification is unknown, but the most common ones include retained fetal bone and osseous metaplasia of endometrial tissue. Calcification appear as hyperechoic area on ultrasound but the gynecologist should also be aware of other differential diagnosis of endometrial ossification which includes mixed Mullerian mesenchymal tumor (MMMT), IUCD, Osseous metaplasia or endometrial tuberculosis. Hysteroscopy is gold standard as diagnostic and therapeutic method.
Retained fetal bone as an entity is not adequately reported in the literature. Prolonged retention of intrauterine bone is recognized as a cause of secondary infertility. One study reported that retained fetal bones may act as an intrauterine synechia or intrauterine device, increasing endometrial prostaglandin F2-alpha and preventing implantation, resulting in infertility (1). The reported incidence is 0.15% at diagnostic hysteroscopy (2). These patients may present with pelvic pain, dysmenorrhea, abnormal uterine bleeding and infertility (3). Apart from retained intrauterine, endometrial calcified lesions and the presence of ectopic bones can also occur by metaplasia in association with chronic inflammation and tissue destruction, mostly presented after repeated spontaneous or therapeutic abortion (4-6).
A Procedure of termination of a pregnancy can at times result in unwanted immediate complications like hemorrhage, uterine perforation, cervical injury and at times in late complications like infections, bleeding, menstrual abnormalities and uterine synechia. As 50% of patients undergoing medical termination are young adults, there is a possibility of secondary infertility due to an abortion that has become complicated (7).
Occasionally if the abortion is done in the second trimester or if the fetus was removed by destructive means, some parts of the fetus may inadvertently be left in the uterine cavity, these could cause pelvic pain, abnormal uterine bleeding, infection, dyspareunia or even vaginally expulsion of fetal bones (8). Few reports have been published describing secondary infertility after abortion. It is expected that retained fetal bones would induce a uterine reaction in the form of vaginal discharge and pain in the majority of such patients while also leading to secondary infertility.
We are presenting the case of a young female who had secondary infertility without any other associated complaints. She had a previous second-trimester abortion four years ago. shad failed to conceive again after previous curettage. Retained fetal bone was confirmed by histopathological analysis of bone fragment collected by hysteroscopy.
Case presentation
A 34 years old lady G4 P3 Ab1, presented in our office with secondary infertility. She had cesarean section delivery 3 times, according to the patient she had a history of an illegal termination of pregnancy at about 4th months of gestation by dilatation and curettage four years before. Following the abortion, she experienced abnormal uterine bleeding for several months and thereafter she could not conceive again. Even she had experienced vaginal expulsion of fetal bones several days after the curettage.
Her vital signs were within the normal range. Pelvic examination was done vaginally and abdominally, both of these were unremarkable.
She had hysteron-sonography revealed a 20 mm linear shadowing, T-shape echogenic lesion like an Intra Uterine Contraceptive Device (IUCD) in the endometrial cavity. Also, there was a 13 × 10 mm echogenic polyp in the posterior fundal wall.
One of the differential diagnosis in the imaging evaluation is osseous metaplasia which can deeply embedded in the endometrium. But considering hysteroscopy findings and pathology report confirmed retained fetal bone. Under general anesthesia, a diagnostic hysteroscopy was performed that showed the presence of a bone (Figure 3) in the uterine cavity. Removal of the bony products and polypectomy was performed by hysteroscopy. On hysteroscopy evaluation there was bony structure which was lying freely in the uterine cavity and separated from underlying tissue and suggestive of bone-like structures in the uterus.
The extracted material was sent for histopathological examination. The pathology report was as follow: specimen received in formalin and consists of several soft irregular yellowish tissues with a little hard area aggregating to 3×1.8×0.8 cm/GH submitted in toto in 1 block. The histopathologic findings are consistent with endometrial polyp, few fragments of endometrium with proliferative pattern and degenerated fragments of bone trabeculae infiltrated by neutrophils. Necrosis and dead bone were observed in pathology, retained fetal bone confirmed.
The Post-operative recovery was unremarkable and subsequent menstrual function was normal.
Discussion
While termination of pregnancy (abortion) is usually a safe procedure, sometimes it has its own complications. Incomplete evacuation of the uterus can result in multiple complications including the rare complication of secondary infertility as presented by us in this case.
Many women with retained fetal bone will have symptoms of menometrorrhagia, dysmenorrhea, vaginal discharge, pelvic pain and spontaneous elimination of bony fragments during the menses in addition to their infertility (9).
Previously published case reports are suggestive that retained fetal bones may be responsible for secondary infertility (6,7,10).
The risk of infertility depends on the location of the retained pieces of bone, whether it is embedded in the myometrium or in the endometrial cavity. There is some evidence that the presence of an intramural bony fragment per se does not seem to compromise fertility if it is completely embedded (9) However commonly, it is speculated Retained fetal bone has been thought to act as a ‘uterine synechia’ or IUCD in the uterine cavity and prevent implantation (1, 10, 11).
Several theories for formation osseous metaplasia cited that previously, endometrial stroma is capable of cartilaginous metaplasia (18). Another hypothesis is that heteroplasia may occur in the multipotential stroma cells present in the uterus thereby forming osseous tissue (12).
In terms of observing hyperechoic area on ultrasound, the gynecologist should be aware of other differential diagnosis of endometrial ossification which includes IUD, osseous metaplasia and fetal retained bone. It is also possible that the presence of bones near the fundal region (where blastocyst implantation mostly takes place) can lead to the elevation of endometrial prostaglandins (e.g., F2alpha) and thus prevent implantation (1).
In case of a history of previous abortion, the clinician should keep in mind the remote possibility of retained fetal bones as a cause of infertility. Transvaginal ultrasonography must be performed in all cases and if any suspicious echoes are seen a hysteroscopy should be planned.
Hystero-sonography allows a detailed visualization of the uterine cavity in both longitudinal and transverse planes, and the endometrium can be evaluated for the presence of polyps, submucous fibroids, intrauterine synechiae and foreign bodies (13).
Hysteroscopy has both accurate diagnostic and therapeutic values. Hysteroscopic removal of the bony pieces should be regarded as the gold standard of treatment since it enables a complete removal of the bones under direct vision.
In terms of pathology, minimal adjacent endometrial reaction with endochondral ossification may help to distinguish osseous metaplasia from retained fetal osteoblastic tissue after an abortion.
Conclusion
Considering that most reports of retention of fetal bones have been in patients with second trimester abortions, routine transvaginal ultrasound to evaluate the completeness of evacuation is suggested. Hysteroscopy guided removal of bony fragments is the gold standard and leads to complete resolution of symptoms.
Sources / references

Fig.1-Hysterosonography revealed calcified intrauterine foreign body, which is suggestive of a retained fetal bone in this case

Fig.2-Hysterosonography: Retained fetal bone which mimics IUD
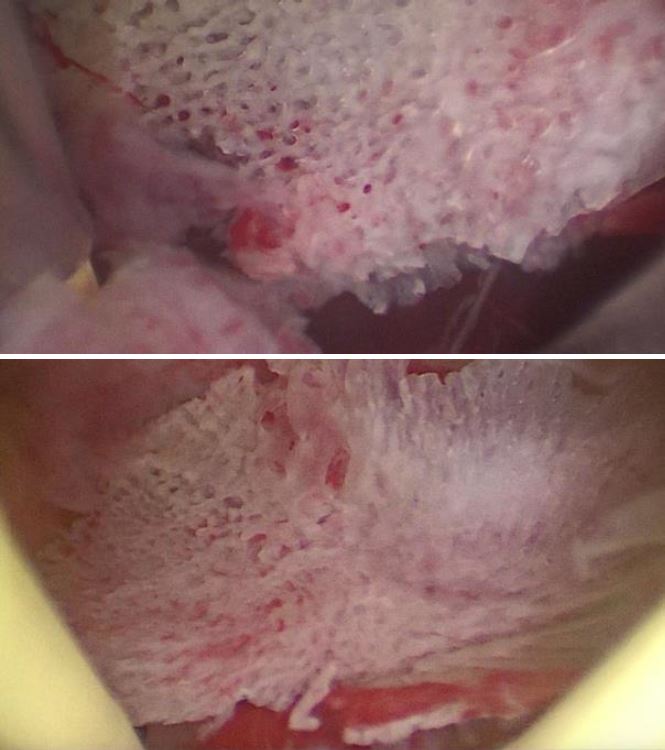
Fig.3-Hysteroscopy view of retained fetal bone
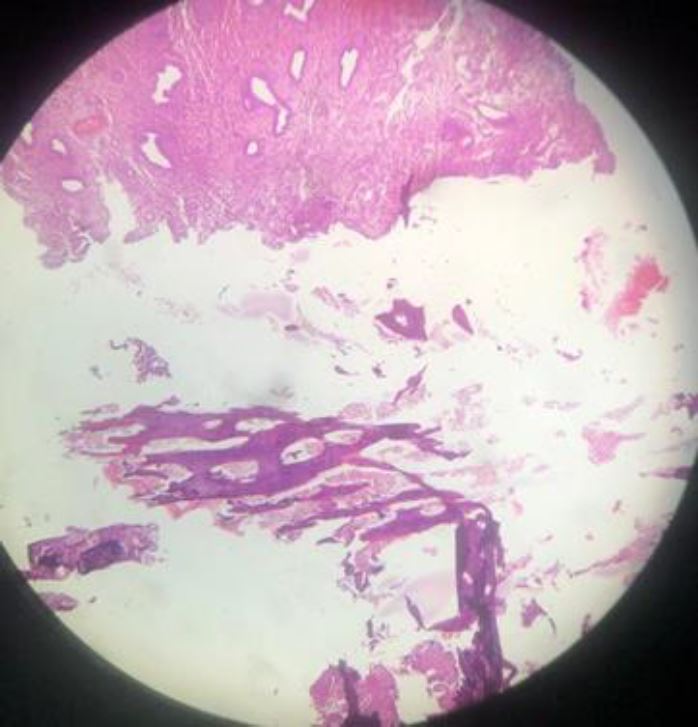
Fig.4 100x magnification of H&E histopathology photomicrograph of uterine content showing sponge bone fragments with bone marrow and secretory phase endometrium
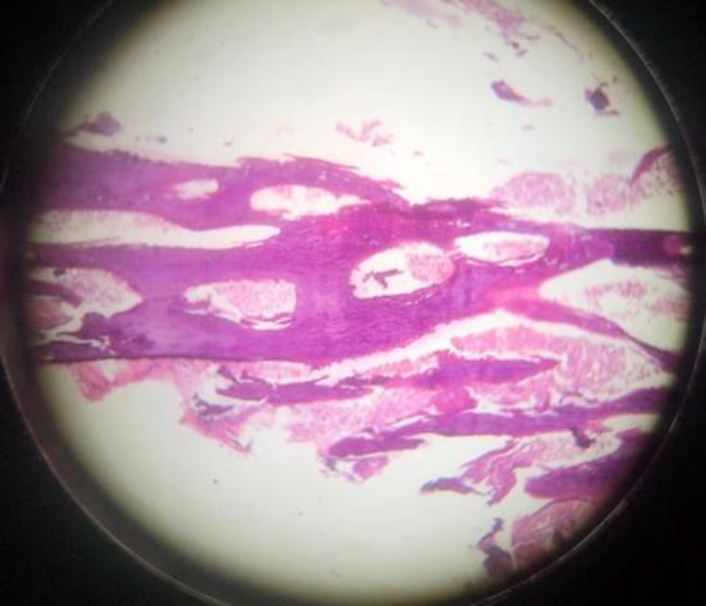
Fig.5-400x magnification of H&E histopathology photomicrograph of uterine content showing sponge bone fragments with bone marrow



