Information
- Author: M. Schettini
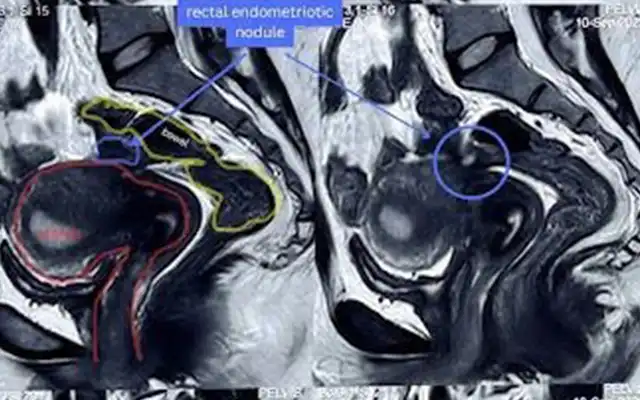
- The ureterocele is a cystic dilatation of the terminal ureter: its formation probably results from incomplete dissolution of Chwalle’s membrane, an embryonic structure that transiently divides the early ureteric bud from the urogenital sinus. Others hypothesises theorize that the condition comes from an abnormal muscular development or from an obstructive condition with mucosal prolapse through the ureteral meatus. The dilatation affects only the terminal tract of the ureter whose protrusion pulls the contiguous bladder wall.
The ureterocele can be mono or bilateral, can manifest in duplex, ectopic or normal ureters and can cause an obstacle to the ureteric voiding.
The cystoscopic appearance of the ureterocele is marked by rhythmical bulking of the sac caused by the force of the urinary flow. Often it is possible to localize the very narrow ureteric meatus where the urinary flow comes from. The urinary stasis in the ureterocele or in the ureter can cause urinary tract infections and stones formation in the ureterocelic sac.
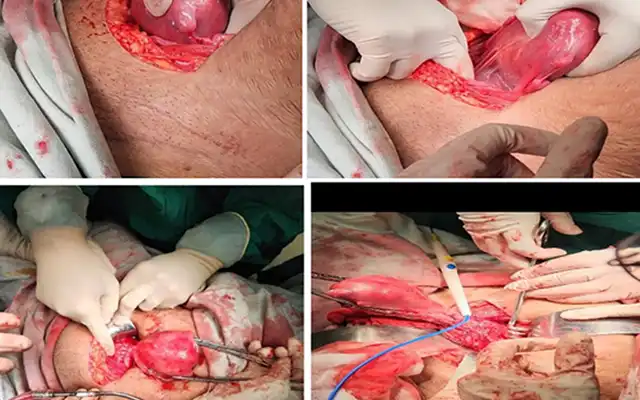
The treatment, without associated pathology of the ureter or the kidney, consists of endoscopic incision and resection of the sac and liberation of ureteric meatus. The treatment of possible ureteric reflux is carried out with endoscopic submucosal injection of bulking agents.
Our cystoscopic technique consists in incising the ureterocele at is maximum bulking with a Collins electrode. The incision is made equatorially and allows the complete opening of the sac; the ureteral meatus is now visible and the urinary flow is free in bladder. Thereafter with a loop electrode all the tissue of the ureterocelic wall is resected. At the end of the procedure the normal position and morphology of the right ureteral meatus is visible.
Video
MEMBERS AREA
Categories